Blood pressure (BP) is the amount of pressure exerted on artery walls during contraction and relaxation of the heart. This pressure is essential for blood to travel throughout the body. BP readings are measured in millimeters of mercury (mm Hg) and are written as systolic pressure (the force the blood is exerting against the artery walls when the heart beats) over diastolic pressure (the force the blood is exerting against the artery walls while the heart is resting between beats). Therefore, a BP reading of 120/80 mm Hg (or verbalized as 120 over 80) tells us that the systolic pressure is 120 mm Hg and the diastolic pressure is 80 mm Hg. A normal BP reading is typically defined as less than 120/80 mm Hg.
Our bodies have a sophisticated way of constantly monitoring BP with specialized mechanoreceptors called baroreceptors (see image below), which then provide information about BP to the autonomic nervous system. There are two types of baroreceptors: high-pressure arterial baroreceptors and low-pressure volume receptors. Both types of baroreceptors are stimulated by the stretching of vessel walls. Arterial baroreceptors are located within the carotid sinuses, which are at the base of the internal carotid arteries in the neck and the arch of the aorta. Low-pressure volume receptors, also known as cardiopulmonary receptors, are located within the atria, ventricles, and pulmonary vasculature (Al-Khazraji and Shoemaker 2018). The arterial baroreceptors are the terminals of afferent fibers that run in the glossopharyngeal and vagus nerves. Rapid decreases in BP result in decreased stretching of the artery wall and a decreased rate of impulse firing from the baroreceptors. This ultimately results in increased cardiac output and vasoconstriction that cause BP to increase. The opposite is found to be true if BP rises rapidly.
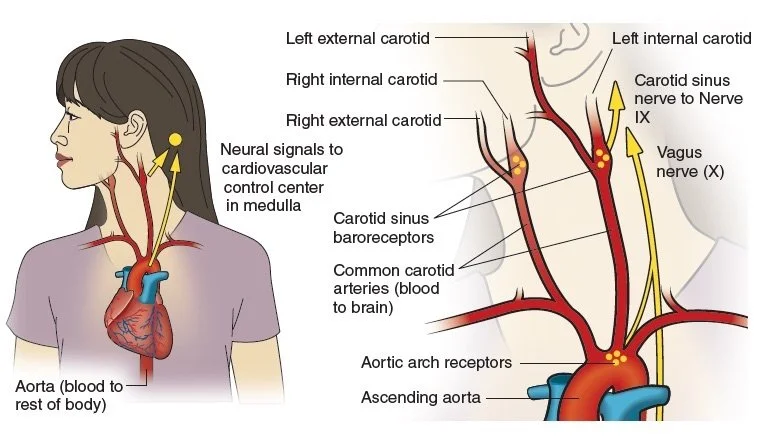
Location of baroreceptors
High BP, known as hypertension, is when blood pressure is consistently too high. The primary way that hypertension causes harm is by increasing the workload of the heart and blood vessels, making them work harder and less efficiently. Over time, the force and friction of hypertension damages the delicate endothelium of the arteries. In turn, this can signify the start of a process called atherosclerosis (explored later in the section on cardiovascular disease).
Essential hypertension, a rise in blood pressure of undetermined cause, includes 90 percent of all hypertensive cases (Messerli, Williams, and Ritz 2007). Strong evidence points to a causal link between a chronically high salt intake and the development of hypertension (Meneton et al. 2005). Additional factors, such as obesity, diabetes, aging, emotional stress, sedentary lifestyle, and low potassium intake may increase the probability of developing hypertension (Takahashi et al. 2011).
Previous guidelines set the BP threshold at 140/90 mm Hg for people younger than 65 years of age and 150/80 mm Hg for those ages 65 and older. In 2017, new guidelines lowered the numbers for the diagnosis of hypertension to 130/80 mm Hg and higher for all adults. These new guidelines stem from the results of the Systolic Blood Pressure Intervention Trial (Whelton et al. 2018) where the results found that aiming for a systolic pressure of no more than 120 mm Hg significantly reduced the chance of heart attacks, heart failure, or stroke over a three-year period.
A reading of 130/80 mm Hg and higher is considered stage 1 hypertension, while a reading of 140/90 mm Hg or higher is considered stage 2 hypertension. Anything higher than 180/120 mm Hg is termed a hypertensive crisis. According to a report by Kearney and colleagues (2005), the total number of adults with hypertension in 2025 is predicted to increase to 1.56 billion worldwide.
A systematic review and meta-analysis by Hagins and colleagues (2013) reported that yoga can be preliminarily recommended as an effective intervention for reducing BP. It is worth noting, however, that most published yoga and BP studies were not randomized, had inadequately described yoga or control programs, did not collect information on other lifestyle factors, and did not use standardized, reliable outcome measures. Additional rigorous controlled trials are warranted to further investigate this benefit of yoga.

The effects of yoga on blood pressure
The precise mechanisms by which yoga practices affect blood pressure currently remain unclear, although it has been proposed that yoga practices lower blood pressure by improving the sensitivity of baroreceptors and chemoreceptors, increasing vagal tone, and decreasing sympathetic nervous system drive. Small changes in BP are therefore detected sooner and controlled more quickly and effectively. In a small study by Vijayalakshmi and colleagues (2004), the authors concluded that yoga optimized the sympathetic response to stressful stimuli and restored the autonomic regulatory reflex mechanisms in hypertensive patients. Another small study by Selvamurthy and colleagues (1998) concluded that yoga training resulted in an improvement of baroreceptor sensitivity. Slow breathing, which is a very significant element of many yogic practices, has been shown to improve arterial baroreflex sensitivity and decrease BP in essential hypertension (Bernardia et al. 2001; Joseph et al. 2005). In a randomized controlled trial by Schneider and colleagues (1995), Transcendental Meditation more significantly reduced systolic and diastolic BP values than a control program. This tells us that the meditative element of yogic practices may also be playing a very significant role in lowering BP. Studies have shown that the medial prefrontal cortex and anterior cingulate gyrus are activated during attention-focusing tasks (Posner and Petersen 1990), and there is also evidence suggesting that a specific relationship between frontal lobe activity and BP exists (Williamson, McColl, and Mathews 2004). It is therefore fair to conclude that the focus that is inherently incorporated into all yogic practices is also significant here. While there is widespread belief that supine and inverted postures in yoga specifically stimulate the baroreceptor reflex, there is surprisingly very little research on this topic. A few studies several decades ago began to explore this (Cole 1989; Razin 1977; Tai and Colaco 1981) but it is challenging to find more recent literature that expands upon this topic.
Yoga students with hypertension that is well controlled can typically practice in the same way as someone with normal BP. If you have uncontrolled hypertension, it is important to get the go-ahead by your health care practitioner before practicing yoga. Students with uncontrolled high blood pressure need to be particularly mindful when it comes to inversions, because elevating the heart above the head and the torso and legs above the heart raises BP. A partially inverted posture like Downward Facing Dog (Adho Mukha Svanasana), where the heart is only slightly above the head and the legs are not elevated, may only slightly increase BP. There are many modifications for Downward Facing Dog that can be adopted, particularly if the student feels too much pressure in their head or feels short of breath. Supported Bridge Pose (Setu Bandha Sarvangasana), lying on bolsters with legs horizontal and feet at hip level increases BP a little more. We will explore these yoga asanas in more detail later in the book. Students should always be given the option to come out of the asana if they feel uncomfortable in any way. Full inversions including Shoulder Stand (Salamba Sarvangasana) and Headstand (Sirsasana) should be avoided when a student has uncontrolled high blood pressure.
References:
Al-Khazraji, B., and J. Shoemaker. 2018. “The Human Cortical Autonomic Network and Volitional Exercise in Health and Disease.” Applied Physiology, Nutrition, and Metabolism 43 (11): 1122-1130.
Bernardia, L., A. Gabuttia, C. Portaa, and L. Spicuzza. 2001. “Slow Breathing Reduces Chemoreflex Response to Hypoxia and Hypercapnia and Increases Baroreflex Sensitivity.” Journal of Hypertension 19:2221-2229.
Cole, R. 1989. “Postural Baroreflex Stimuli May Affect EEG Arousal and Sleep in Humans.” Journal of Applied Physiology 67 (6): 2369-2375.
Hagins, M., R. States, T. Selfe, and K. Innes. 2013. “Effectiveness of Yoga for Hypertension: Systematic Review and Meta-Analysis.” Evidence-Based Complementary and Alternative Medicine 2013: 649836.
Joseph, C., C. Porta, G. Casucci, N. Casiraghi, M. Maffeis, M. Rossi, and L. Bernardi. 2005. “Slow Breathing Improves Arterial Baroreflex Sensitivity and Decreases Blood Pressure in Essential Hypertension.” Hypertension 46 (4): 714-718.
Kearney, P., M. Whelton, K. Reynolds, P. Muntner, P. Whelton, and J. He. 2005. “Global Burden of Hypertension: Analysis of Worldwide Data.” Lancet 365 (9455): 217-223.
Meneton, P., X. Jeunemaitre, H. de Wardener, and G. MacGregor. 2005. “Links Between Dietary Salt Intake, Renal Salt Handling, Blood Pressure, and Cardiovascular Diseases.” Physiology Reviews 85 (2): 679-715.
Messerli, F., B. Williams, and E. Ritz. 2007. “Essential Hypertension.” Lancet 370 (9587): 591-603.
Posner, M., and S. Petersen. 1990. “The Attention System of the Human Brain.” Annual Review of Neuroscience 13:25-42.
Razin, A. 1977. “Upside-Down Position to Terminate Tachycardia of Wolff-Parkinson-White Syndrome.” New England Journal of Medicine 296 (26): 1535‐1536.
Schneider, R., F. Staggers, C. Alexander, W. Sheppard, M. Rainforth, K. Kondwani, S. Smith, and C. King. 1995. “A Randomised Controlled Trial of Stress Reduction for Hypertension in Older African Americans.” Hypertension 26 (5): 820-857.
Selvamurthy, W., K. Sridharan, U. Ray, R. Tiwary, K. Hegde, U. Radhakrishan, and K. Sinha. 1998. “A New Physiological Approach to Control Essential Hypertension.” Indian Journal of Physiology and Pharmacology 42(2): 205-213.
Tai, Y., and C. Colaco. 1981. “Upside-Down Position for Paroxysmal Supraventricular Tachycardia.” Lancet 2(8258): 1289.
Takahashi, H., M. Yoshika, Y. Komiyama, and M. Nishimura. 2011. “The Central Mechanism Underlying Hypertension: A Review of the Roles of Sodium Ions, Epithelial Sodium Channels, the Renin-Angiotensin-Aldosterone System, Oxidative Stress and Endogenous Digitalis in the Brain.” Hypertension Research 34 (11): 1147-1160.
Vijayalakshmi, P., Madanmohan, A.B. Bhavanani, A. Patil, and K. Babu. 2004. “Modulation of Stress Induced by Isometric Handgrip Test in Hypertensive Patients Following Yogic Relaxation Training.” Indian Journal of Physiology and Pharmacology 48:59-64.
Whelton, P., R. Carey, W. Aronow, D. Casey, K. Collins, C. Dennison Himmelfarb, S. DePalma, S. Gidding, K. Jamerson, D. Jones, et al. 2018. “2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults.”Journal of the American College of Cardiology 71 (19): e127-e248.
Williamson, J., R. McColl, and D. Mathews. 2004. “Changes in Regional Cerebral Blood Flow Distribution During Postexercise Hypotension in Humans.” Journal of Applied Physiology 96 (2): 719-724.